

Is It Safe to Drive While Stoned? Cannabis and Driving
An Erowid Science Review
v1.0 - Feb 4, 20101
Citation: Sewell RA. "Is It Safe to Drive While Stoned? Cannabis and Driving: An Erowid Science Review". Erowid.org. Feb 4, 2010. Erowid.org/plants/cannabis/cannabis_driving7.shtml
Introduction
It is often difficult to get reliable information on the effects cannabis use has on driving. The purpose of this review is not to answer this question, but rather to summarize the scientific research on the subject so drivers can make their own educated decisions; and also to look at how scientists go about answering this difficult question.Accidents are the fifth leading cause of death in the United States; nearly half are motor vehicle accidents, which killed 34,017 people in 2008 alone.2 Motor vehicle accidents are the leading cause of death in those under 30.4 The death rate for teenagers is four times that of drivers age 25 to 69, and a quarter of all traffic deaths are in drivers under age 25.6 Characteristics associated with dying in a car accident are being a young man who is thrill-seeking, overconfident, drives too fast, late at night, in an unfamiliar vehicle, while not wearing a seatbelt, or any combination of the above.7 A quarter of all traffic deaths involve a driver with a blood alcohol level of 0.01 g/dL (one eighth the legal limit) or more, and in 21-year-old drivers, the intoxicated dead account for four in ten.8 Drivers with a previous DWI ("Driving While Impaired") conviction were responsible for 7.2% of all crashes involving alcohol.8
The percentage of road traffic accidents in which one driver tested positive for cannabis ranges widely in published reports, from 6% to 32%.
More people have been smoking cannabis in recent years, because it's easy to find, cheaper, more potent,16 and more socially acceptable than it used to be.17 Most smokers start at age 18, and ten years later, 8% of users have lost control of their cannabis use.18 However, most people smoke cannabis only once in a while for a short period of time, generally stop in their mid-to-late 20s, and only a few smoke every day for long periods.19
As cannabis is the most commonly used illegal drug--an estimated 40% of the population (12 and older) has tried it20--and is also smoked most commonly in the age group that also has the most road traffic accidents, a considerable amount of research has been done to see if cannabis smoking causes more road traffic accidents. Since cannabis is not very toxic by itself, dying in a car accident is probably the worst thing that can happen to cannabis smokers--another reason to study the question. So, how safe is smoking and driving?
That's a question that's difficult to answer because it's so vague. Scientists have approached the problem by breaking it down into four more specific questions:
- Does cannabis affect the brain circuitry you need to drive safely?
- Does cannabis use impair performance on driving tests?
- When two cars crash, is the person responsible for the crash more likely to be under the influence of cannabis?
- Do cannabis smokers die in car crashes more often than non-cannabis smokers?
Cognitive studies: Does cannabis affect the brain circuitry you need to drive safely?
Cannabis affects attentiveness, vigilance, time perception, speed perception, and use of acquired knowledge.21-24 In fact, a meta-analysis (a way of combining lots of smaller studies to make one larger and more powerful study) of 60 studies concluded that cannabis causes impairment in almost every performance area connected with safe driving--such as tracking, motor coordination, visual functions, and complicated tasks that require divided attention.25 The most problems are found with attention, tracking, and psychomotor skills, with the worst impairment concentrated in the first two hours after smoking. It's not clear what cannabis's effect is on reaction time.26 Other reviewers agree with this assessment.4 Worse still, when used together, the negative effects of cannabis and alcohol seem to add together or even synergize.27 If cognitive studies were the only studies done, it would be clear that smoking cannabis increases the risk of having a fatal traffic accident.Driving and simulator studies: Does cannabis use impair performance on driving tests?

Photo from Colorado State University |
Some scientists have suggested that the reason why stoned drivers do not crash more in laboratory simulations or road tests, even though they are clearly impaired, is because cannabis users tend to think they are more stoned than they really are, and do their best to compensate for it. In contrast, drunk drivers typically think they are less drunk than they really are. Given a dose of 7 mg THC (about a third of a joint), drivers rated themselves as impaired even though their driving performance was not. In contrast, at a blood alcohol concentration of 0.04% (slightly less than two cans of beer; half the legal limit in most US states), driving performance was impaired even though drivers rated themselves as fine.31 Cannabis smokers think they are driving badly when they are stoned and they also drive more cautiously.31-34
What do scientists mean by cautiously? Stoned drivers increase their following distance, try to overtake less, and drive more slowly. The opposite is true of drunk drivers.34 One review of eight driving simulator studies and seven on-road studies35 found that smoking cannabis was associated with either poor lane control31,36-39 or slower driving that successfully maintained lane control.40-42 In seven of ten studies cited in that review, the stoned drivers drove more slowly even through they were given explicit instructions to maintain a faster speed, and a more recent simulator study published in 2008 found the same thing.43 Two simulator studies showed that the tendency to overtake was decreased with cannabis use but increased with alcohol.44,45 One simulator study and two on-road studies found that cannabis smokers tend to increase the distance between themselves and the car in front of them.31,36 Other studies have found that cannabis use does not impair sign detection,40 a sudden lane-changing task,34 or detecting and responding to hazardous events.39
In seven of ten studies cited in one review, the stoned drivers drove more slowly even through they were given explicit instructions to maintain a faster speed, and a more recent simulator study published in 2008 found the same thing.
Meta-analyses of over 120 studies have found that in general, the higher the estimated concentration of THC in blood, the worse the driving, but that people who smoke all the time show less impairment than infrequent users at the same dose. This may be from physiological tolerance (in the same way that heavy drinkers can "hold their liquor") or because they have simply learned how to function while stoned. The worst driving impairment is found 20 to 40 minutes after smoking, but people are usually back to normal 2.5 hours later, at least in those who smoke 18 mg THC or less (the dose often used experimentally to duplicate a single joint).50,51
Interestingly, three reports indicate that chronic cannabis smokers are less affected by alcohol on some measures than nonsmokers or infrequent smokers. As far back as 1970, the famous psychoactive drug researcher Dr. Reese Jones noticed that alcohol had less of an effect in heavy cannabis smokers.52 A study twenty years later showed that regular cannabis smokers show less impairment in peripheral signal detection when drunk than infrequent users do,53 and a later study still found that regular cannabis users given just alcohol show less decrease in tracking accuracy and lower dizziness ratings than infrequent users given the same amount of alcohol.54 It is unclear why this is. It is possible that there is "cross-tolerance" between cannabis and alcohol on a physiological level. It may also be that people who have learned to function in one altered state of consciousness can also function better in another.
Cannabis use increases reaction time and the number of incorrect responses to emergencies.
One weakness of driving studies is that subjects know that they are being observed and rated, so they do their best to drive well. However, safe driving depends not only on ability, but also behavior, and things like thrill-seeking, road rage, and risk-taking tend not to show themselves in simulated and on-road tests. These studies are a better measure of what drivers are capable of doing rather than what they actually do, so they might underestimate the risk. Data from actual road accidents are necessary to determine what people actually do.
Epidemiological studies try to measure the actual risk that a driver may cause an accident under the influence of a drug, relative to that of a sober person driving under similar conditions. The relative risk is expressed in the form of an "odds ratio" (OR), which is the multiplier for the increased accident risk from driving under the influence of cannabis. For example, an odds ratio of 2.0 means that being stoned doubles the risk of experiencing the outcome in question, which is usually either having a car crash, being judged responsible for a car crash, or being killed in a car crash. An OR of 1.0 would mean no effect, and an OR of 0.5 would mean that the risk is cut in half. Epidemiologists take two different approaches. The first is culpability studies, which classify drivers who have crashed according to their degree of responsibility (culpability) for the crash, then compare cannabis use in each category. If there is greater use of cannabis in those responsible for the crash, then cannabis use is judged to cause a greater crash risk. The second is case control studies. We will discuss both in turn.
| What's the difference between delta9-THC and carboxy-THC? |
 The chemical delta9-tetrahydrocannabinol (delta9-THC or THC), which is present in cannabis, is the primary chemical responsible for making people feel stoned. It peaks in the blood within minutes but 90% is gone in an hour.
The chemical delta9-tetrahydrocannabinol (delta9-THC or THC), which is present in cannabis, is the primary chemical responsible for making people feel stoned. It peaks in the blood within minutes but 90% is gone in an hour. Delta9-THC is metabolized into 11-OH-THC (11-hydroxy-THC or THC-carboxylic acid), which also contributes to the high. This lingers for hours in the blood and is also absorbed up by fat cells to last even longer in the body.
Delta9-THC is metabolized into 11-OH-THC (11-hydroxy-THC or THC-carboxylic acid), which also contributes to the high. This lingers for hours in the blood and is also absorbed up by fat cells to last even longer in the body. This metabolite, 11-hydroxy-THC, is further metabolized into THC-COOH (carboxy-THC), which leaves the body in urine. Carboxy-THC is not psychoactive, can take as long as four hours to appear in the urine, and can take weeks to be eliminated fully from the body. Confusingly, all three molecules are abbreviated "THC", which leads to a lot of muddled conversations about how long THC lasts in the body.
This metabolite, 11-hydroxy-THC, is further metabolized into THC-COOH (carboxy-THC), which leaves the body in urine. Carboxy-THC is not psychoactive, can take as long as four hours to appear in the urine, and can take weeks to be eliminated fully from the body. Confusingly, all three molecules are abbreviated "THC", which leads to a lot of muddled conversations about how long THC lasts in the body.You can see why measuring carboxy-THC is a bad way to tell if someone's stoned. Not only does it not answer the question, it actually muddles the issue. Unfortunately, blood tests for delta9-THC didn't become available until 1998, so before then, that was what scientists used. |
Culpability studies: When two cars crash, is the person responsible for the crash more likely to be under the influence of cannabis?
Some reviewers have concluded that not only does driving stoned not increase the culpability for crashes, it may actually reduce risk.57 Dr. Drummer's review of blood samples of traffic fatalities in Australia found that drivers testing positive for cannabis were actually less likely to have been judged responsible for the accident.58 Several other studies have also found no increase in crash risk with cannabis.59-61 Dr. Williams' California study of 440 male traffic accident deaths found that while alcohol use was related to crash culpability, cannabis use was not.62 Dr. Terhune's study of 1882 motor vehicle deaths calculated an OR of 0.7 for cannabis use, 7.4 for alcohol use, and 8.4 for cannabis and alcohol use combined.59 Dr. Lowenstein and Dr. Koziol-McLain's study of 414 injured drivers admitted to a Colorado emergency department found an OR of 1.1, which--statistically speaking--indicates that cannabis use was not really associated with increased crash responsibility.63 Dr. Drummer's later and more extensive ten-year study of 3,400 traffic fatalities in three Australian states found the following:| Cannabis-Related Blood Levels | Odds Ratio (OR) for Crash Death |
|---|---|
| Only carboxy-THC present | 1.0 |
| THC < 5 ng/dL | 1.0 |
| THC > 5 ng/dL | 6.6 |
By comparison, a blood alcohol level of 0.15% (almost twice the legal limit in most states) also causes an OR of 6.6. In fact, in all of the 30 cases in this study in which one driver had a serum level of THC greater than 10 ng/mL, that driver was judged to have been responsible for the accident. When cannabis was combined with alcohol, the risk was higher still.64
A later reanalysis of the same data that adjusted for the age and sex of the fatalities found that OR of crashing while being stoned (but on nothing else) dropped to 0.6 (not statistically different from 1.0 in this case), versus 7.6 for alcohol.57 Dr. Laumon's study of 10,748 French motor vehicle fatalities found that although rates of stoned driving or drunk driving were similar (nearly 3%), ten times as many fatal crashes were associated with alcohol as with cannabis. Like Dr. Drummer, he noted that the higher the THC levels in the blood, the more the crash risk, and calculated an OR of 4.7 for THC levels greater than 5 ng/mL, similar to Dr. Drummer's calculation of 6.6.65 Dr. Longo's large, well-known study of hospitalized injured drivers in South Australia showed that driving stoned didn't affect crash risk overall, although he too found that there was a slightly higher risk of crashing with higher THC concentrations and a slightly lower risk with lower concentrations.66
| What does it mean to "adjust for age and sex"? |
| Let's suppose you wanted to figure out who played basketball better, men or women, so you took a group of men at random and a group of women at random, and found that the men won more games than the women. You might conclude that men are better basketball players than women. Not so fast! Men are also taller on average than women, and we know that helps in basketball. Suppose you repeat the experiment, now matching men and women of equal height, and discovered that men and women now won an equal number of games? You would have found that an apparent difference in basketball between men and women disappears when controlling for height. In practice, scientists don't have to repeat the experiment; they can do it statistically, as long as they can think of what the third factor might be. If wearing eyeliner makes it hard to play basketball and women were more likely to wear eyeliner, and the experimenter didn't realize this or think to control for it, then the false conclusion would stand. |
What do the blood levels mean?
What does "5 ng/mL" mean in terms of actual impairment? It's hard to calculate, as THC blood levels peak quickly after smoking then drop rapidly in a complicated way, unlike alcohol levels, which makes it almost impossible to calculate backwards from the concentration of THC at the time of the blood test to the concentration at the time of the traffic accident. When 1,276 stoned Swedish motorists were arrested for DUI the average THC blood level was 3.6 ng/mL at the time of testing.67 A similar Swiss study of 440 stoned DUI suspects found average blood concentrations of 5.0 ng/mL at the time of testing, showing that 5 ng/mL found later seems to go along with bad driving spotted earlier.68 Of 291 DUI arrestees in the Swedish study who were positive for both THC and alcohol, the average THC blood level was only 2.3 ng/mL, again suggesting that when combined with alcohol, it doesn't take as much cannabis to cause impairment obvious to police.67 A Norwegian study that looked to see how many of 589 cannabis-positive drivers arrested by police were rated as "clinically impaired" by the police doctor found that half of those judged impaired had a THC blood level above 2.5 ng/mL, and half below, and the ratings of impairment increased considerably above 3.0 ng/mL.69As with all scientific studies, there are some "gotchas". Urine stays positive for carboxy-THC long after the effects of cannabis wear off, so studies that use carboxy-THC to classify drivers as cannabis users will mistakenly include some un-stoned drivers with the stoned ones--making cannabis seem safer than it actually is.70 The Colorado study that found that cannabis was not associated with increased crash responsibility used urine toxicology to assess drug use, so probably made this mistake.63 A wait of longer than an hour between arrest and blood test can make the THC concentration in the blood of injured drivers who test positive for cannabis seem lower than it is, possibly explaining Dr. Longo and others' failure to find adverse effects. (Of course, THC does not degrade in the blood of a dead person, so studies of motor vehicle fatalities don't have that problem.)
| Blood Levels and Subjective Effects Alcohol vs. Cannabis |
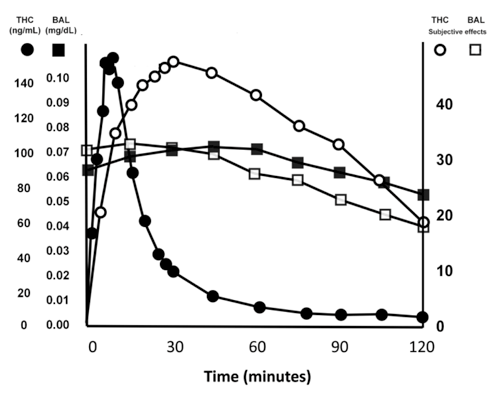 Figure 2: Serum levels of ethanol (black squares) lag behind subjective effects (white squares) because tolerance develops very quickly. Subjective effects of THC (white circles) lag behind serum levels (black circles) because THC moves into the brain more slowly than alcohol does. BAL=Blood Alcohol Level. (Adapted from Portans et al. (1989),1 Cocchetto et al. (1981),3 Huestis et al. (1992).5) |
In contrast to the above studies, several other studies that have found that cannabis users are almost twice as likely to be responsible for crashes (OR 1.7).72-74 Dr. Crouch found that cannabis use contributed to the demise of 168 fatally injured truckers in all cases in which the serum concentration of THC exceeded 1 ng/mL.75 Dr. Terhune's study of 497 road traffic accidents found that cannabis users had a responsibility rate of 76% versus 42.5% for the non-smokers.76 A later, larger study by the same author of 1,882 drivers killed in seven US states found no difference between responsibility rates, however,59 and it is unclear why the conclusions of his two studies were different.
Unfortunately, many studies that point the finger at cannabis don't take into account other drugs on board at the same time,72-74 and since alcohol and cannabis together are worse than either drug alone, not taking drinking into account exaggerates the role played by cannabis. What's more, if the people who are assigning culpability for the accident know the results of the blood test, they are more likely to blame the accident on the cannabis smoker, all else being equal, making the argument that cannabis use contributed to the accident a circular one. Scientists can only draw conclusions about the effects of cannabis use on culpability when the people assigning culpability are "blinded"--do not know who was using cannabis. This was likely the problem with Dr. Crouch's study.75
In summary, although culpability studies seem to contradict each other somewhat, all agree that combining alcohol and cannabis has worse consequences than use of cannabis alone.59,62,64,77 In general, culpability studies suffer from three main weaknesses. The first is the delay between accident and blood sampling, which mistakenly classifies some THC users who were impaired at the time of the accident into the non-use group; the second is use of the metabolite carboxy-THC to identify cannabis-users, which can mistakenly classify some non-impaired drivers in the impaired group; and the third is use of raters who knew who had smoked cannabis before determining blame.
Case-control studies: Do cannabis-smokers die in car crashes more often than non-cannabis smokers?
In contrast with culpability studies, case control studies compare the prevalence of cannabis use among drivers injured or killed in traffic accidents with a "control group"--or comparison group--of other drivers. The trick with these studies is in selecting the appropriate control group.One case-control study by Dr. Movig and his team in the Netherlands found an OR (odds ratio--remember; risk multiplier) of 1.2--no statistically meaningful association--between smoking cannabis and crashing, even when they did not control for use of other drugs.78 In fact, a preliminary analysis by the same group that did control for other drugs initially generated an OR of 0.3, indicating that cannabis use actually decreased crash risk.79 A recent study by Dr. Jones in Australia also found no increase in the number of accidents that cannabis smokers had in the previous year compared with controls.80
In contrast, some case-control studies have found increased risk. Dr. Gerberich, in a large retrospective study of 64,657 health plan members in Northern California, found an OR of 2.3 for motor vehicle injuries among male cannabis users versus nonusers.81 Dr. Mura's French study of injured drivers in the emergency room calculated an OR of 2.5 for cannabis users versus sober controls, which rose to 4.6 when alcohol was combined with cannabis.82 Drs. Dussault and Brault's study comparing THC in the blood or carboxy-THC in the urine of traffic fatalities with similar tests of drivers in a roadside survey calculated an OR of 2.2 for cannabis use leading to fatal injury.83,84 Another study of 30,896 traffic fatalities found that of the 1,647 in which cannabis was present in the blood, cannabis use was associated with an OR of 1.29 for a potentially unsafe driving behavior preceding the crash.85 Interestingly, in this study Dr. Bedard found no difference in rates of failure to stay within lane between cannabis smokers and non-smokers, contradicting the findings of several laboratory simulator studies.56,86 Finally, one last study by Dr. Haworth in Australia of 127 single-vehicle crashes within 200 km of Melbourne found an amazingly high OR of 38 for crashing after smoking!87
Case-control studies are valid only if the cases are properly matched with comparison controls, which is hard to do.
It is because of problems like these that epidemiological studies contradict each other, some finding decreased or no risk from driving while smoking cannabis, and others increased risk. Most studies have had designs that led to underreporting of cannabis use or misclassification of drivers into or out of the cannabis-using category, making a mess of the results.
So what can we say for sure?
Although from the results of studies on brain circuitry you would think that cannabis use leads to unsafe driving, simulator and on-road studies have suggested that it can have the opposite effect. Epidemiological studies (culpability and case-control) contradict each other. One possible explanation for all this confusion is that people who smoke cannabis share qualities--being young, male, and risk-taking--that would make them more likely to have car accidents even if they didn't smoke cannabis. For example, smoking cannabis goes along with speeding,88 drunk driving, and not wearing a seatbelt.89 Some researchers have suggested that there is a single factor--perhaps a "risky behavior" characteristic or "general driving problem" that underlies all risky driving behaviors, including driving stoned.90,91 If that's the case, then cannabis smoking while driving is a symptom, not a cause--people who choose to smoke pot and then get behind the wheel tend to be bad drivers anyway!Two epidemiological studies in New Zealand that looked at this question found that the relationship that existed between self-reported cannabis use and self-reported accidents (OR 1.6 and 3.9, respectively) disappeared after they controlled for risky driver behaviors and "unsafe driver attitudes".92,93 A follow-up study found that the OR for crashing (2.3) when driving under the influence of cannabis more than 20 times in one year was halved--reduced to marginal significance--when researchers controlled for distance driven and self-reported risky driving behaviors. This particular study used 12 driving violations including: exceeding the speed limit by more than 20 kph; driving without a seat belt; deliberately driving through red lights; street racing; driving without a license; driving when the license had been suspended; driving without a current vehicle registration; driving without a current vehicle warrant of fitness; changing lanes without signaling; overtaking without a clear view of the road ahead; overtaking illegally; and driving too close to other vehicles.94
A third Canadian study that looked at crash rates in cannabis users found an even higher adjusted OR of 2.61 for crashing over the course of the year in those who drove while "stoned" versus cannabis smokers who did not, suggesting that people who decide to drive even when they're stoned have poor judgment and unsafe driving habits (and therefore higher crash risk) even when they're not stoned.95 And a Montreal study published this summer studied the driving behavior of cannabis smokers in a simulator when they weren't stoned.96 Dr. Richer, the lead investigator, found that young male cannabis smokers, 80% of whom had driven stoned in the last year, had high rates of risky and dangerous driving (speeding, overtaking illegally, passing in the right lane, omitting stops, etc.) and negative emotional driving ("road rage"), all of which would lead to more accidents even if they didn't smoke cannabis before they drove. The men who drove stoned also tended to be younger, more impulsive, and more sensation-seeking. This has led some researchers to suggest that the increased risk of crashing by stoned drivers is because of the "characteristics of the young people who used cannabis rather than the effects of cannabis use on driver performance."92
Some researchers suggest that the increased risk of crashing by stoned drivers is because of the "characteristics of the young people who used cannabis rather than the effects of cannabis use on driver performance."92
Combining cannabis with alcohol is a double whammy, however, resulting in bad driving at doses so small that people would be fine to drive if they had taken either drug by itself. Case-control studies contradict each other, but it seems that while low concentrations of THC do not increase the rate of accidents, and may even decrease them, blood levels of THC higher than 5 ng/mL increase the risk of accidents (Figure 2). Overall, though, case-control and culpability studies contradict each other enough that it's hard to say anything for sure, and other reviewers agree.97,98 By comparison, similar disagreement among scientists has never existed on the link between drinking alcohol and crash risk.99
Recommendations
Although, as you can see, scientists have been unable to answer definitively whether or not it is safe to drive while stoned, we have learned something from all this, and based on what is known we can make some recommendations.Cannabis users should:
- Have a "designated driver" or take a taxi, just as they would if they were drinking alcohol.
- Wait at least three hours after smoking before driving, if they can't avoid driving.
- Never mix alcohol and cannabis before driving, since the combination is much more dangerous than either drug by itself.
- Remember that cannabis makes monotonous, prolonged driving particularly difficult.
- Not let being stoned allow them to forget to wear a seatbelt.
References #
- Portans I, White J, Staiger P. "Acute Tolerance to Alcohol: Changes in Subjective Effects Among Social Drinkers". Psychopharmacology. 1989;97:365-9. [ Abstract ]
- National Highway Traffic Safety Administration. Fatality Analysis Reporting System (FARS). In: National Center for Statistics and Analysis. 2008. [ Source ]
- Cocchetto DM, Owens S, Perez-Reyes M, et al. "Relationship Between Plasma Delta-9-Tetrahydrocannabinol Concentration and Pharmacologic Effects in Man". Psychopharmacology. 1981;75:158-64. [ Abstract ]
- Centers for Disease Control and Prevention. Web-Based Injury Statistics Query and Reporting System (WISQUARS). In: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. 2008. [ Source ]
- Huestis M, Henningfield J, Cone E. "Blood Cannabinoids. I. Absorption of THC and Formation of 11-OH-THC and THCCOOH During and After Smoking Cannabis". J Anal Toxicol. 1992;16:276-82. [ Abstract ]
- National Highway Traffic Safety Administration. Traffic Safety Facts 2000: A Compilation of Motor Vehicle Crash Data from the Fatality Analysis Reporting System and the General Estimates System. Washington, DC: National Center for Statistics and Analysis, U.S. Department of Transportation. 2001. [ Full Text ]
- World Health Organization. World Report on Road Traffic Injury Prevention. Geneva, Switzerland: World Health Organization. 2004. [ Full Text ]
- Subramanian R. Alcohol Involvement in Fatal Motor Vehicle Traffic Crashes, 2003. Springfield, VA: National Highway Traffic Safety Administration (NHTSA). 2005. [ Full Text ]
- van den Bree MB, Pickworth WB. "Risk Factors Predicting Changes in Marijuana Involvement in Teenagers". Arch Gen Psychiatry. 2005;62:311-9. [ Abstract ]
- McLean S, Parsons RS, Chesterman RB, et al. "Drugs, Alcohol and Road Accidents in Tasmania". Med J Aust. 1987;147:6-11. [ Abstract ]
- Soderstrom CA, Dischinger PC, Kerns TJ, et al. "Marijuana and Other Drug Use Among Automobile and Motorcycle Drivers Treated at a Trauma Center". Accid Anal Prev. 1995;27:131-5. [ Abstract ]
- Alvarez FJ, Fierro I, Del Rio MC. "Cannabis and Driving: Results from a General Population Survey". Forensic Sci Int. 2007;170:111-6. [ Abstract ]
- Albery IP, Strang J, Gossop M, et al. "Illicit Drugs and Driving: Prevalence, Beliefs and Accident Involvement Among a Cohort of Current Out-of-treatment Drug Users". Drug Alcohol Depend. 2000;58:197-204. [ Abstract ]
- Macdonald S, DeSouza A, Mann R, et al. "Driving Behavior of Alcohol, Cannabis, and Cocaine Abuse Treatment Clients and Population Controls". Am J Drug Alcohol Abuse. 2004;30:429-44. [ Abstract ]
- Terry P, Wright KA. "Self-reported Driving Behaviour and Attitudes Towards Driving Under the Influence of Cannabis Among Three Different User Groups in England". Addict Behav. 2005 ; 30:619-26. [ Abstract ]
- ElSohly M, Ross S, Mehmedic Z, et al. "Potency Trends of Delta-9-THC and other Cannabinoids in Confiscated Cannabis from 1980-1997". J Forensic Sci. 2000;45:24-30. [ Abstract ]
- Dennis M, Babor TF, Roebuck MC, et al. "Changing the Focus: The Case for Recognizing and Treating Cannabis Use Disorders". Addiction. 2002;97:Suppl 1. [ Abstract ]
- Wagner FA, Anthony JC. "From First Drug Use to Drug Dependence; Developmental Periods of Risk for Dependence Upon Cannabis, Cocaine, and Alcohol". Neuropsychopharmacology. 2002;26:479-88. [ Abstract ]
- Bachman DS. "Smoking Cessation via Telephone Counseling & Tools for Helping Your Patients Quit Smoking Once and for All". The Journal of the Arkansas Medical Society. 1997;94:147-8.
- Office of Applied Studies. Results from the 2005 National Survey on Drug Use and Health: National Findings. Rockville, MD: Substance Abuse and Mental Health Services Administration. 2006. [ Full Text ]
- Moskowitz H. "Marihuana and Driving". Accid Anal Prev. 1985;17:323-45. [ Abstract ]
- Hall W. "The Health and Psychological Consequences of Cannabis Use". Canberra: Australian Government Publication Service. 1994.
- Kurzthaler I, Hummer M, Miller C, et al. "Effect of Cannabis Use on Cognitive Functions and Driving Ability". J Clinical Psychiatry. 1999;60:395-9.
- Liguori A, Gatto CP, Robinson JH. "Effects of Marijuana on Equilibrium, Psychomotor Performance, and Simulated Driving". Behavioural Pharmacology. 1998;9:599-609. [ Abstract ]
- Berghaus G, Guo B. "Medicines and Driver Fitness--Findings from a Meta-analysis of Experimental Studies as Basic Information to Patients, Physicians and Experts". In: Kloeden C, McLean A; Alcohol, Drugs, and Traffic Safety--T95: Proceedings of the 13th International Conference on Alcohol, Drugs and Traffics Safety 1995 Adelaide, Australia. 1995;295-300.
- Foltin R, Evans S. "Performance Effects of Drugs of Abuse: A Methodological Survey". Human Psychopharmacology. 1993;8:9-19. [ Abstract ]
- Chesher G. "The Effects of Alcohol and Marijuana in Combination: A Review". Alcohol, Drugs and Driving. 1986;2:105-19.
- Robbe H. Influence of Cannabis on Driving. Maastricht, The Netherlands: University of Limburg. 1994. [ Full Text ]
- Smiley A. "Cannabis: On-Road and Driving Simulator Studies". In: Kalant H, Corrigal W, Hall W, et al., eds. The Health Effects of Cannabis. Toronto: Centre for Addiction and Mental Health. 1998.
- Sutton LR. "The Effects of Alcohol, Marihuana and their Combination on Driving Ability". J Studies on Alcohol. 1983 ; 44:438-45. [ Abstract ]
- Robbe H, O'Hanlon J. Marijuana and Actual Driving Performance. Washington, DC: US Department of Transportation, National Highway Traffic Safety Administration. 1993. [ Full Text ]
- MacDonald S, Mann R, Chipman M, et al. "Driving Behavior Under the Influence of Cannabis or Cocaine". Traffic Inj Prev. 2008;9:190-4. [ Abstract ]
- Hindrik W, Robbe J, O'Hanlon J. Cannabis, Alcohol, and Actual Driving Performance. Washington, DC: National Highway Traffic Safety Administration, US Department of Transportation. 1999. [ Full Text ]
- Smiley A. "Cannabis: On-road and Driving Simulator Studies". Alcohol, Drugs and Driving. 1986;2:121-34.
- Smiley A. "Cannabis: On-Road and Driving Simulator Studies". In: Kalant H, Corrigal W, Hall W, Smart R, eds. The Health Effects of Cannabis. Toronto: Addiction Research Foundation. 1999;173-91.
- Smiley A, Moskowitz H, Ziedman K. "Driving Simulator Studies of Cannabis Alone and in Combination with Alcohol". In: 25th Conference of the American Association for Automotive Medicine 1981. 1981;107-16.
- Klonoff H. "Cannabis and Driving in Real-life Situations". Science (New York, NY). 1974;186:317-24. [ Abstract ]
- Hansteen RW, Miller RD, Lonero L, et al. "Effects of Cannabis and Alcohol on Automobile Driving and Psychomotor Tracking". Annals of the New York Academy of Sciences. 1976;282:240-56. [ Abstract ]
- Sexton B, Tunbridge R, Brook-Carter N, et al. The Influence of Cannabis on Driving. Crowthorne, UK: TRL Limited. 2000.
- Stein A, Allen R, Cook M, et al. A Simulator Study of the Combined Effects of Alcohol and Cannabis on Driving Behavior. Systems Technology, Inc. 1983.
- Peck R, Biasotti A, Boland P, et al. "The Effects of Cannabis and Alcohol on Actual Driving Performance". Alcohol, Drugs and Driving: Abstracts and Reviews. 1986;2:135-54.
- Casswell S. "Cannabis and Alcohol: Effects on Closed-course Driving Behavior". In: 7th International Conference on Alcohol, Drugs, and Traffic Safety 1979 Melbourne, Australia. 1979.
- Ronen A, Gershon P, Drobiner H, et al. "Effects of THC on Driving Performance, Physiological State and Subjective Feelings Relative to Alcohol". Accid Anal Prev. 2008;40:926-34. [ Abstract ]
- Dott A. Effect of Cannabis on Risk Acceptance in a Simulated Passing Task. Washington, DC: US Government Printing Office. 1971.
- Ellingstad V, McFarling L, Struckman D. Alcohol, Cannabis and Risk Taking. Vermillion, DS: Vermillion Human Factors Laboratory, South Dakota University. 1973.
- Crancer A Jr, Dille JM, Delay JC, et al. "Comparison of the Effects of Marihuana and Alcohol on Simulated Driving Performance". Science (New York, NY). 1969;164:851-4. [ Abstract ]
- Rafaelsen L, Christrup H, Bech P, et al. "Effects of Cannabis and Alcohol on Psychological Tests". Nature. 1973;242:117-8. [ Abstract ]
- Moskowitz H, Hulbert S, McGlothlin W. "Cannabis: Effects on Simulated Driving Performance". Accid Anal Prev. 1976;8:45-50.
- Casswell S. "Cannabis and Alcohol: Effects on Closed-course Driving Behavior". In: Johnson I, ed.. Seventh International Conference on Alcohol, Drugs, and Traffic Safety 1977 Melbourne, Australia. 1977;238-46.
- Kruger H. [Low Alcohol Concentrations and Driving]. Bergisch Gladbach: Bundesanstalt f�r Strassenwesen. 1990.
- Berghaus G. ["Comparison of the Effects of Cannabis and Alcohol from Experimental Studies"]. In: Grotenhermen F, Karus M, eds. [Cannabis, Driving and Workplace]. Heidelberg/New York: Springer Verlag. 2002;225-35.
- Jones RT, Stone GC. "Psychological Studies of Marijuana and Alcohol in Man". Psychopharmacologia. 1970;18:108-17.
- Marks DF, MacAvoy MG. "Divided Attention Performance in Cannabis Users and Non-users Following Alcohol and Cannabis Separately and in Combination". Psychopharmacology. 1989;99:397-401. [ Abstract ]
- Wright A, Terry P. "Modulation of the Effects of Alcohol on Driving-related Psychomotor Skills by Chronic Exposure to Cannabis". Psychopharmacology. 2002;160:213-9. [ Abstract ]
- Sexton B, Tunbridge R, Board A, et al. The Influence of Cannabis and Alcohol on Driving. Crowthorne, UK: Transport Research Laboratory. 2002.
- Ramaekers JG, Robbe HW, O'Hanlon JF. "Cannabis, Alcohol and Actual Driving Performance". Hum Psychopharmacol. 2000;15:551-8. [ Abstract ]
- Bates MN, Blakely TA. "Role of Cannabis in Motor Vehicle Crashes". Epidemiologic Reviews. 1999;21:222-32.
- Drummer OH. "A Review of the Contributions of Drugs in Drivers to Road Accidents". In: Inquiry into the Effects of Drugs (Other than Alcohol) on Road Safety in Victoria, Incorporating Selected Papers. Melbourne, Australia: LV North, Government Printer. 1995;1-28.
- Terhune K, Ippolito C, Hendricks D, et al. The Incidence and Role of Drugs in Fatally Injured Drivers. Washington, DC: National Highway Traffic Safety Administration, U.S. Department of Transportation. 1992.
- Drummer OH. "Drugs and Accident Risk in Fatally Injured Drivers". In: T95: 13th International Conference on Alcohol, Drugs and Traffic Safety 1995 Adelaide, Australia. 1995.
- Terhune K. "An Evaluation of Crash Culpability to Assess Alcohol and Drug Impairment Effects". In: 26th Annual Meeting, American Association for Automotive Medicine 1982 Ontario, Canada. 1982.
- Williams AF, Peat MA, Crouch DJ, et al. "Drugs in Fatally Injured Young Male Drivers". Public Health Rep. 1985;100:19-25. [ Abstract ]
- Lowenstein SR, Koziol-McLain J. "Drugs and Traffic Crash Responsibility: A Study of Injured Motorists in Colorado". J Trauma. 2001;50:313-20. [ Abstract ]
- Drummer OH, Gerostamoulos J, Batziris H, et al. "The Involvement of Drugs in Drivers of Motor Vehicles Killed in Australian Road Traffic Crashes". Accid Anal Prev. 2004;36:239-48. [ Abstract ]
- Laumon B, Gadegbeku B, Martin JL, et al. "Cannabis Intoxication and Fatal Road Crashes in France: Population Based Case-control Study". BMJ (Clinical Research Ed). 2005;331:1371. [ Abstract ]
- Longo MC, Hunter CE, Lokan RJ, et al. "The Prevalence of Alcohol, Cannabinoids, Benzodiazepines and Stimulants Amongst Injured Drivers and their Role in Driver Culpability: Part II: The Relationship Between Drug Prevalence and Drug Concentration, and Driver Culpability". Accid Anal Prev. 2000 ; 32:623-32. [ Abstract ]
- Jones AW, Holmgren A, Kugelberg FC. "Driving Under the Influence of Cannabis: A 10-Year Study of Age and Gender Differences in the Concentrations of Tetrahydrocannabinol in Blood". Addiction. 2008;103:452-61. [ Abstract ]
- Augsburger M, Donze N, Menetrey A, et al. "Concentration of Drugs in Blood of Suspected Impaired Drivers". Forensic Sci Int. 2005;153:11-5. [ Abstract ]
- Khiabani HZ, Bramness JG, Bjorneboe A, et al. "Relationship Between THC Concentration in Blood and Impairment in Apprehended Drivers". Traffic Inj Prev. 2006;7:111-6. [ Abstract ]
- Grotenhermen F, Leson G, Berghaus G, et al. "Developing Limits for Driving Under Cannabis". Addiction. 2007;102:1910-7. [ Abstract ]
- Papafotiou K, Carter JD, Stough C. "The Relationship Between Performance on the Standardised Field Sobriety Tests, Driving Performance and the Level of Delta9-tetrahydrocannabinol (THC) in Blood". Forensic Sci Int. 2005;155:172-8. [ Abstract ]
- Simpson HM, Mayhew DR, Warren RA. "Epidemiology of Road Accidents Involving Young Adults: Alcohol, Drugs and Other Factors". Drug Alcohol Depend. 1982;10:35-63. [ Abstract ]
- Simpson HM. "Epidemiology of Road Accidents Involving Cannabis". Alcohol, Drugs and Driving. 1986;2:15-30.
- Warren RA, Simpson HM, Hilchie J, et al. "Drugs Detected in Fatally Injured Drivers in the Province of Ontario". In: Goldberg L, ed. Alcohol, Drugs and Traffic Safety. Stockholm, Sweden: Almqvist and Wiksell International. 1981;203-17.
- Crouch DJ, Birky MM, Gust SW, et al. "The Prevalence of Drugs and Alcohol in Fatally Injured Truck Drivers". J Forensic Sci. 1993;38:1342-53. [ Abstract ]
- Terhune K. "Problems and Methods in Studying Drug Crash Effects". Alcohol, Drugs and Driving. 1986;2:1-13.
- Hunter CE, Lokan RJ, Longo M, et al. The Prevalence and Role of Alcohol, Cannabinoids, Benzodiazepines and Stimulants in Non-fatal Crashes. Adelaide, Australia: Forensic Science, Department for Administrative and Information Services. 1998.
- Movig KL, Mathijssen MP, Nagel PH, et al. "Psychoactive Substance Use and the Risk of Motor Vehicle Accidents". Accid Anal Prev. 2004;36:631-6. [ Abstract ]
- Mathijssen MP, Movig KL, De Gier JJ, et al. "Use of Psychoactive Medicines and Drugs as a Cause of Road Trauma". In: 16th International Conference on Alcohol, Drugs and Traffic Safety T2002 2002 Montreal, Canada. 2002;451-8.
- Jones C, Donnelly N, Swift W, et al. "Driving Under the Influence of Cannabis: The Problem and Potential Countermeasures". Crime and Justice Bulletin. 2005;87:1-15. [ Full Text ]
- Gerberich SG, Sidney S, Braun BL, et al. "Marijuana Use and Injury Events Resulting in Hospitalization". Annals of Epidemiology. 2003;13:230-7. [ Abstract ]
- Mura P, Kintz P, Ludes B, et al. "Comparison of the Prevalence of Alcohol, Cannabis and Other Drugs between 900 Injured Drivers and 900 Control Subjects: Results of a French Collaborative Study". Forensic Sci Int. 2003;133:79-85. [ Abstract ]
- Dussault C, Brault M, Bouchard J, et al. "The Contribution of Alcohol and Other Drugs Among Fatally Injured Drivers in Quebec: Some Preliminary Results". In: 16th International Conference on Alcohol, Drugs and Traffic Safety T2002 2002 Montreal, Canada. 2002;423-30. [ Full Text ]
- Brault M, Dussault C, Bouchard J, et al. "The Contribution of Alcohol and Other Drugs Among Fatally Injured Drivers in Quebec: Final Results". In: T2004: 17th International Conference on Alcohol, Drugs and Traffic Safety 2004 Glasgow, UK. 2004.
- Bedard M, Dubois S, Weaver B. "The Impact of Marijuana on Driving". Canadian Journal of Public Health. 2007;98:6-11. [ Abstract ]
- Robbe H, O'Hanlon J. Marijuana and Actual Driving Performance: National Highway Traffic Safety Administration, U.S. Department of Transportation. 1993. [ Full Text ]
- Haworth N, Vulcan P, Bowland L, et al. Fatal Single Vehicle Crashes Study: Summary Report (No. 122). Melbourne, Australia: Monash University Accident Research Center. 1997. [ Source ]
- Vassallo S, Smart D, Sanson A, et al. "Risky Driving Among Young Australian Drivers II: Co-occurrence with Other Problem Behaviours". Accid Anal Prev. 2008;40:376-86. [ Abstract ]
- Everett SA, Lowry R, Cohen LR, et al. "Unsafe Motor Vehicle Practices Among Substance-using College Students". Accid Anal Prev. 1999;31:667-73. [ Abstract ]
- Fergusson D, Swain-Campbell N, Horwood J. "Risky Driving Behaviour in Young People: Prevalence, Personal Characteristics and Traffic Accidents". Aust N Z J Public Health. 2003;27:337-42. [ Abstract ]
- Jonah B. "Psychosocial Characteristics of Impaired Drivers: An Integrated Review in Relation to Problem Behavior Theory". In: Wilson R, Mann R, eds. Drinking and Driving: Advances in Research and Prevention. New York: Guilford Publications, Inc. 1990. [ Abstract ]
- Fergusson DM, Horwood LJ. "Cannabis Use and Traffic Accidents in a Birth Cohort of Young Adults". Accid Anal Prev. 2001;33:703-11. [ Abstract ]
- Blows S, Ivers RQ, Connor J, et al. "Cannabis Use and Car Crash Injury". Addiction (Abingdon, England). 2005;100:605-11. [ Abstract ]
- Fergusson DM, Horwood LJ, Boden JM. "Is Driving Under the Influence of Cannabis Becoming a Greater Risk to Driver Safety than Drink Driving? Findings from a longitudinal study". Accident Analysis and Prevention. 2008;40:1345-50. [ Abstract ]
- Mann RE, Adlaf E, Zhao J, et al. "Cannabis Use and Self-reported Collisions in a Representative Sample of Adult Drivers". J Safety Res. 2007;38:669-74. [ Abstract ]
- Richer I, Bergeron J. "Driving Under the Influence of Cannabis: Links with Dangerous Driving, Psychological Predictors, and Accident Involvement". Accid Anal Prev. 2009;41:299-307. [ Abstract ]
- Kelly E, Darke S, Ross J. "A Review of Drug Use and Driving: Epidemiology, Impairment, Risk Factors and Risk Perceptions". Drug Alcohol Rev. 2004;23:319-44. [ Abstract ]
- Beirness D, Simpson H, Williams A. "Role of Cannabis and Benzodiazepines in Motor Vehicle Crashes". Transportation Research Circular. 2006;E-C096:12-21. [ Full Text ]
- Moskowitz H. "Commentary on Variability Among Epidemiological Studies of Drugs and Driving". Transportation Research Circular. 2006;E-C096:36-40. [ Full Text ]
Image Credits #
- Example of a driving simulator. Photo from Colorado State University Driving Simulator Facility.
- Blood Levels and Subjective Effects: Alcohol vs. Cannabis. Graph by RA Sewell, adapted from Portans et al. 1989, Cocchetto et al. 1981, and Huestis et al. 1992.
Revision History #
- Different Article - May-Jun 2009 - Sewell RA et al. - A different article based on Sewell's review work appeared in The American Journal on Addictions.
- v1.0 - Feb 2010 - Sewell RA - Published on Erowid.org.