

How Do They Measure Up?
Examining Drug Use Surveys and Statistics, Part I: The Sources
Nov 2005
Citation: Erowid E, Erowid F. "How Do They Measure Up? - Part I: Examining Drug Use Surveys and Statistics". Erowid Extracts. Nov 2005;9:12-15.
see also: Part II: The Problems
Every few weeks Americans are treated to startling new statistics about drug use, from an alarming increase in the abuse of prescription drugs by women to an encouraging decrease in the use of marijuana by teens. The announcements ripple across the country, carried by newspapers and reported on the evening news.
The announcements are discussed by government officials in press releases and by parents in arguments with their children. They are also cited by lawmakers in debates on the floors of legislatures and by judges in the highest courts.1
But where do the original statistics come from? What do we really know about the rates of drug use in the United States and around the world?
National and international "drug use" statistics are commonly cited when discussing the medical, social, legal, and political aspects of psychoactive drugs. These statistics are used to justify large expenditures, draconian punishments, and a substantial amount of public and government attention on the unapproved use of psychoactives.The announcements are discussed by government officials in press releases and by parents in arguments with their children. They are also cited by lawmakers in debates on the floors of legislatures and by judges in the highest courts.1
But where do the original statistics come from? What do we really know about the rates of drug use in the United States and around the world?
Despite these important uses, there is no accurate and practical way to measure levels of illegal or disapproved drug use across large populations. Most of the statistics are gleaned from a handful of surveys that ask respondents about their own use. These results are interesting, but are based on indirect data that can be affected by a wide variety of factors. It is thus unclear how well such surveys measure actual psychoactive use.
Types of Data
Four major survey types and several additional primary data sources are used to estimate rates of unapproved psychoactive substance use. Each provides its own benefits and challenges. It is useful to keep in mind the types of data that are being collected and compare the problems and benefits associated with each type.In-Person Household Surveys
Household surveys are conducted in the homes of those being surveyed. Homes are selected based on demographics. Phone calls are made ahead of time to establish that someone in the household meets survey criteria, and then an appointment is made. Participation is voluntary, although some pressure is applied to get chosen households to participate.The survey usually includes an oral question segment as well as a computer or pencil-and-paper portion filled out by the respondent. Though anonymity is assured by the surveyor, there is conflicting evidence about whether participants feel they are secure.2,3
Phone Household Surveys
These surveys are conducted with individuals over the phone while they are in their homes. Homes are selected based on demographics. Phone calls are made to find someone at home who fits the study criteria and agrees to answer questions. Participation is voluntary with some pressure applied, usually in the form of multiple calls made. Interestingly, phone surveys may be experienced as less confidential than in-person surveys.4In-School Surveys
Surveyed are conducted in classrooms or, less frequently, auditoriums. Schools and classes are chosen to fit the study criteria. Participation is theoretically voluntary, though there may be significant pressure to participate by those in positions of authority within the school. Nearly all in-school surveys are anonymous, written instruments that involve no direct questions by a surveyor. These are considered more anonymous than other survey types because they are taken and submitted in groups.Testing of Italy's Po River found high levels of a cocaine metabolite, benzoylecgonine.11 Researchers believe this results from the urine of cocaine users in the surrounding valley. The levels found suggest a much higher level of cocaine consumption in the valley than had previously been estimated.
Arrestee or Jail Surveys
Individuals who have been arrested are asked questions about their psychoactive use. They may also be asked to submit a urine sample, which is tested and used to verify their responses. Jail surveys include otherwise difficult-to-survey populations and are one of the few survey types that validates at least a portion of answers (via urinalysis). Most are anonymous and voluntary, though they may not appear so to respondents.Medical Data
Information about patients' drug use is collected from emergency rooms, medical examiners and addiction treatment centers. Data may include difficult-to-survey populations. Data is not connected to individual patients, but is used without patient consent.Law Enforcement Data
Data from law enforcement sources includes numbers of drug-related arrests and convictions as well as quantities of drugs seized at borders and during raids. Data may include difficult-to-survey populations and is used without the consent of arrestees.Other Data
A variety of other data types can be used to estimate or validate use rates: street availability, price and purity; physical data showing environmental levels of drugs or their by-products (such as the presence of cocaine on paper currency); or records of precursor sales used to estimate production rates.
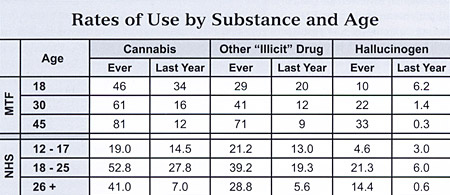 Monitoring the Future, through in-school and follow-up surveys, has found that 81% of 45-year-olds in the United States say they have tried cannabis and 88% have tried cannabis or another illicit drug. The National Household Survey finds slightly lower numbers in all age groups.5,6 |
Monitoring the Future
With nearly 50,000 responses in 2004, Monitoring the Future (MTF) is the second largest psychoactive drug usage survey in the United States. MTF uses mostly in-school surveys of 14- to 18-year-olds enrolled in middle and high school. Funded by the U.S. Federal Government, it has been conducted every year since 1975.
MTF researchers publish extensive discussions of the problems with their methods and how they adjust their numbers to try to account for known weaknesses. Because of the in-school design, MTF is able to achieve a relatively low miss/refusal rate of 17% of selected subjects, lower than most other surveys.
Perhaps the most interesting feature of the MTF survey is that it conducts follow-up, in-home surveys of a portion of participants who have previously completed in-school surveys. A random subset of high school senior respondents are surveyed every other year until age 30, and then every five years after that. The "retention" rates for follow-up surveys is 50-60%, well below the initial in-school response rates.7
These long-term follow-up surveys, conducted since 1975, represent 30 years of continuous response data about past and current use. This longitudinal data stands out as some of the richest, most interesting information available about drug use.
It is assumed that respondents who later become addicted or chronic users would be much less likely to participate in the follow-up surveys, and the MTF does not attempt to include these people in their estimates: "We believe that people who become dependent on, or addicted to, heroin or cocaine are unlikely to be retained in any reasonable proportions. That is why we are careful to not quantify or characterize these special segments of the population."8
The MTF survey's longitudinal nature also makes it useful for comparing against other survey data. Its reports include comparisons between MTF and the National Household Survey (NHS), including substantial criticism of NHS's methods and conclusions.9 Finally, the MTF's follow-up surveys document the extremely interesting problem of recanting past psychoactive use: some people who previously stated that they had used a psychoactive later say they never have. The "Recanting Effect" is discussed in more depth in Part 2 of this article.
Its long history, longitudinal design, and publication of methodology has made Monitoring the Future perhaps the best source of data about unapproved psychoactive drug use in the United States, if not the world.
National Household Survey
The National Household Survey, recently renamed the National Survey on Drug Use and Health (NHS or NSDUH), is the largest regular survey covering psychoactive drug use. It has been conducted since 1971 and in 2004 had nearly 68,000 responses. The NHS is an in-person household survey that includes questions about mental and general health as well as health insurance and other demographic factors. Homes or apartments are selected using a random sampling technique intended to make the results representative across the United States. Surveyors go to each residence with handheld computers and are trained to convince potential respondents that their answers will be kept confidential.
"Surveyors incorporat[e] procedures that would be likely to increase respondents' cooperation and willingness to report honestly about their illicit drug use behavior. Confidentiality is stressed in all written and oral communications with potential respondents. Respondents' names are not collected."10 After households are selected, the NHS has a miss/refusal rate of about 22.6%, which is surprisingly low considering that surveyors must request to go into people's homes.
The NHS faces many major hurdles involved in collecting reliable data and is assumed to substantially under-represent heavy users and other hard-to-survey populations. The NHS's use estimates are, across the board, substantially lower than those of MTF and other surveys. The NHS includes a detailed description of its survey and statistical methods, but its recent reports are missing many key tables.
The MTF and NSDUH are the Federal Government's largest and primary tools for tracking youth substance use.13
— SAMHSA, Office of Applied Statistics
Unfortunately, due to "important methodological differences" between the most recent survey designs and those from earlier years, it is no longer possible to directly compare use rates over the history of the survey. Differences include the change in the name of the survey, the addition of a $30 incentive payment for respondents, new quality control procedures, and the incorporation of new population data from the 2000 decennial census.
According to the NHS, "The changes resulted in a substantial improvement in the survey response rate [and] also affected respondents' reporting of many critical items that are the basis of prevalence measures reported by the survey each year." It concludes that newer data "should not be compared with 2001 and earlier NHSDA data to assess changes over time."
Drug Abuse Warning Network
Another frequently cited source of drug use statistics is the Drug Abuse Warning Network (DAWN), which is a non-survey data source that uses reports from U.S. hospital emergency departments. DAWN works with a set of U.S. hospitals that agree to fill out forms related to emergency department (ED) admissions. Hospitals are selected in order to create a representative sample allowing DAWN to estimate incidence of drug use emergencies and deaths across the United States. In the second half of 2003, DAWN worked with 518 hospitals, but received useable data from only 260, a 50% response rate. To solve some of the deep methodological problems with the design, DAWN changed and simplified its procedures in 2005.14
Prior to 2005, DAWN procedures were as follows: A designated DAWN "reporter" in each hospital reviewed the charts of all patients treated in the ED--including toxicology test results (blood or urine) and comments by nurses and doctors--or any deaths reviewed by the Medical Examiner/Coroner. The reporters identified cases that involved "drug abuse" matching a two-part definition: 1) the use of an illegal drug, the use of a drug in an unapproved way, or the use of non-medical inhalants, AND 2) the drug was used "because of drug dependence", to attempt suicide, "for recreational purposes or to achieve other psychic effects".
Each identified case (for patients between the ages of 6 and 97) was recorded with demographic information, route of administration, reason for the emergency department visit, reason for using the substance, and a list of up to four identified drugs. It is important to note that a drug did not need to be directly related to the emergency room visit to be listed as a mention. Notably, cases involving alcohol but no other "abused drug" were not included in the DAWN report. Also, cases of "accidental" ingestion or inhalation of a drug with "no intent to abuse" were not considered valid DAWN cases.
In April 2005, DAWN announced "new DAWN", a major revision of its data collection methods, many of which improve how reliably data is collected.15 New DAWN makes reporting far simpler and more reproducible. Any "drug-related" ED visit qualifies, as opposed to only those related to "drug abuse". Reported incidents must be simply be related to "recent drug use" rather than requiring a complicated set of criteria to determine whether drug use was related to the ED event. New DAWN includes anyone of any age and no longer excludes based on intent of use; intent is now entered as a category. Finally, the new format includes more training and feedback between DAWN and cooperating hospitals.
Published DAWN reports warn against extrapolating too much from their data and suggest DAWN's primary purpose is to detect trends. The DAWN incidents are often called "mentions" because the data is usually tabulated by the total number of times a given drug was mentioned. Single individuals may account for more than one DAWN incident each year.
"[A]ccording to the Substance Abuse and Mental Health Services Administration, emergency room mentions for cocaine use have increased from about 80,000 in 1990 to about 161,000 in 1997. Emergency room mentions for heroin grew from about 34,000 in 1990 to 72,000 in 1997. A naive observer might infer that cocaine and heroin use doubled between 1990 and 1997, but this is almost certainly wrong... While DAWN can be very valuable for detecting short-term changes in specific jurisdictions--such as a spike in overdose deaths--it would seem to have little or no value as a tool for monitoring long-term trends in the prevalence of substance abuse."16
— ONDCP
Arrestee Drug Abuse Monitoring
The Arrestee Drug Abuse Monitoring program (ADAM) is the largest drug-related survey of adult arrestees in the United States, with 22,666 responses collected in 2003 (the most recent year of publication). The ADAM program conducts a drug and alcohol use survey of people who have been arrested and booked as adults in city and county detention facilities operated by local police and sheriff departments. The surveys are conducted by civilian (non-police) researchers who choose individuals using a "probability-based sampling" method in an attempt to obtain a representative sample of arrestees. Researchers then do in-person interviews and voluntary urine analysis.
ADAM and other jail surveys are valuable because they collect data samples from populations that are very difficult to survey using other methods. ADAM also uses urinalysis to partially validate survey results. For many substances, this is not terribly effective, but it works well for cannabis as well as for recent use of other drugs.
ADAM's miss/refusal rate of 43.3% (11% active refusal, 32% unavailable for various reasons) complicates extrapolating the data and may further support the notion that some sub-populations are simply extremely difficult to survey. It is unclear how to extrapolate from selected jail arrestees to the wider population.
Canadian Addiction Survey
The phone-based Canadian Addiction Survey (CAS) is one of Canada's first attempts to do ongoing national surveying about psychoactive drug use. There are no major phone-based surveys in the United States. Telephone numbers are selected with an attempt to create a nationally representative sample and voice surveys are performed in either English or French. Eligible respondents are those 15 or older who completed the interview at one of the selected phone numbers.
In 2004, the CAS had a total of 13,909 valid responses with a miss/refusal rate of 54%. This survey has little track record to determine whether its methodology will produce stable results, nor does it involve external validation (verification of actual use). The CAS necessarily only includes populations that have and answer household wired telephones. Because of this, the CAS will, like most other surveys, miss hard-to-survey populations such as addicts, heavy users, and members of transient subcultures, as well as cell-phone-only users. Surveys relying on phones alone as a means of data collection are of unknown validity as measures of actual psychoactive use. The published survey reports do not discuss the impact of the refusal/miss rate on the data.
Law Enforcement Data
Various Sources
A variety of data available from law enforcement organizations is used to detect trends in drug use. Metrics include numbers of drug-related arrests and prosecutions, drug seizures, drug price, and drug purity, and are collected from the DEA, FBI, and Federal Bureau of Prisons, among others. This data is used to help validate survey statistics about drug use and the illegal drug market. There is no single, comprehensive report which gathers or summarizes this information for major law enforcement agencies in the United States.
According to CASA, teens who see three or more R-rated movies each month are "six times likelier to try marijuana".17
The primary methodological difficulty with extrapolating from law enforcement data is that investigations and prosecutions are largely driven by economic, political, and social factors that may have little or no relationship to actual prevalence of use. Law enforcement data can help confirm trends or detect real world rise in certain types of psychoactive drug-related crime, but it is improper to extrapolate from these sources to the wider population. For example, one can easily imagine that arrests and prosecutions may increase because of changes in political climate, while use itself remains constant.
Other Data Sources
Various Sources
Other major sources of information about psychoactive use in the United States:
- The Youth Risk Behavior Surveillance System (YRBSS), a school-based survey sponsored by the Centers for Disease Control with over 15,000 responses in 2003.
- Treatment Episode Data Set (TEDS), a non-representative but huge collection of substance abuse-related admissions to participating clinics with almost two million admissions in 2002. Data is of limited value in estimating usage levels because there is no tracking of individuals; one individual can account for many admissions. Admission rates fluctuate based on space and funding availability and changes in court-, school- or parent-ordered treatment.
- National Longitudinal Study of Adolescent Health (Add Health), an in-school survey of teens with follow-up interviews that provide some longitudinal data.
- Survey of Inmates in State and Federal Correction Facilities (SISFCF), a drug use and health survey of inmates from state and federal prisons.
- National Comorbidity Survey (NCS), a mental health survey looking at mental health issues and "comorbidities" (multiple health problems in the same person that may or may not be related) and including survey questions about psychoactive drug use.
- Department of Defense Survey of Health Related Behaviors Among Military Personnel, the largest survey of military personnel; includes questions about psychoactive drug use. Part of its purpose is to document how well military drug testing programs discourage current use. There are also a number of less scientific or more biased sources of survey data. News media frequently report survey results from political and prohibitionist organizations that do not openly publish their methods and have little scientific validity.
- The Partnership for a Drug Free America, consistently produce breathlessly-worded survey summaries using newly coined phrases and scandalous findings showcasing new drug crises hiding right under our noses.
- The Center on Addiction and Substance Abuse at Columbia University (CASA), a self-described "research center" and highly funded publisher, is one of the most poorly regarded sources of statistics and analysis in the United States. CASA pays marketing firms to conduct small, non-representative sample phone surveys and issues blatantly unscientific reports to bolster highly sensationalized press releases about the dangers of drugs, alcohol, and pre-marital sex. Although it is well liked within the prohibitionist political establishment and continues to receive funding from major foundations, CASA's reports and studies do not rise to the level of source surveys and must be discarded when evaluating drug use statistics.
see also: Part II: The Problems
References #
- Gonzales v. Raich. U.S. S.Ct. 03-1454. Oral Arguments Transcript. 2004. p 35.
- Johnson T, Fendrich M. "Modeling sources of self-report bias in a survey of drug use epidemiology." Ann Epidemiol. 2005;15:381-389.
- O'Malley PM, Johnston LD, Bachman JG, et al. "A comparison of confidential versus anonymous survey procedures." J Drug Issues. 2000;30:35-54.
- Moskowitz JM. "Assessment of cigarette smoking and smoking susceptibility among youth." Public Opin Q. 2004;68(4):565-87.
- Johnston LD, O'Malley PM, Bachman JG, et al. Monitoring the Future National Survey Results on Drug Use, 1975-2004. Vol II. NIDA. 2005. 91.
- Substance Abuse and Mental Health Services Administration. 2004 National Survey on Drug Use & Health: National Findings. 2005. 234-6. Accessed Oct 24 2005, http://www.oas.samhsa.gov/nsduh.htm.
- Johnston LD, O'Malley PM, Bachman JG, et al. Monitoring the Future National Survey Results on Drug Use, 1975-2003. Vol II. NIDA. 2004. 67.
- Johnston, 58.
- Johnston LD, O'Malley PM, Bachman JG, et al. Monitoring the Future National Survey Results on Drug Use, 1975-2003. Vol I. NIDA. 2004.
- SAMHSA. 2003 National Survey on Drug Use & Health. 2003. 90.
- Zuccato E, Chiabrando C, Castiglioni S, et al. "Cocaine in surface waters." Environ Health. Aug 2005;4:14.
- SAMHSA, 2003. 193.
- SAMHSA, 2003. Appendix D.
- Roberts CD. "Data quality of the Drug Abuse Warning Network." Am J Drug Alcohol Abuse. Aug 1996;22(3):389-401.
- "New Dawn: Why It Cannot Be Compared with Old Dawn." The New DAWN Report. DAWN. Sep 2005. Accessed Oct 15 2005 http://dawninfo.samhsa.gov/files/New_DAWN_Reports.htm.
- Rhodes W, Layne M, Johnston P, et al. "What America's Users Spend on Illegal Drugs 1988-1998." ONDCP. Dec 2000. Accessed Oct 19, 2005. http://www.whitehousedrugpolicy.gov/publications/drugfact/american_users_spend/.
- CASA. "Teens Who Watch R-Rated Movies Likelier to Smoke, Drink, Use Marijuana." CASA 2005 Teen Survey. Aug 18, 2005.